Cancer
Net New Zealand
home page
home page
Introduction
In 2003, the United States Environmental Protection Agency (EPA) declared that the link between the chlorination of drinking water and cancer was sufficient to require regulatory action to retire chlorination and replace it with filtration.
The EPA stated:
" III Public Health Risk
Chlorine has been widely used as a chemical disinfectant, serving as a principal barrier to microbial contaminants in drinking water. However, the microbial risk reduction attributes of chlorination have been increasingly scrutinized due to concerns about potential increased health risks ... new health studies continue to support an association between bladder, colon and rectal cancers from long-term exposure to chlorinated surface water. In addition to cancer effects, recent studies have reported associations between use of chlorinated drinking water and a number of reproductive and developmental endpoints including spontaneous abortion, still birth, neural tube defect, pre-term delivery, low birth weight and intrauterine growth retardation (small for gestational age)...Based on the weight of evidence from both the human epidemiology and animal toxicology data on cancer and reproductive and developmental health effects and consideration of the large number of people exposed ... the combined health data warrant regulatory action..." ( Federal Register / Vol.68. No. 159 / Monday, August 18, 2003 / Proposed Rules p. 49557 )
A brief summary of the Cancer and Heart Failure Epidemics
Epidemiologically, the cancer rate doubles in the first 12 months following the start of chlorination of any particular drinking water supply.
Those who die in the first 12 months are mainly in the 70+ age bracket.
Chlorine gas used to treat drinking water produces hypochlorous acid and it is this strong oxidising agent that acts as the disinfectant.
Hypochlorous acid is not selective. As well as oxidising bacteria and killing them, it oxidises human cells causing damage leading to mutation and cancer.
Over the course of a lifetime the consumption of hypochlorous acid in chlorinated water moves the age of cancer initiated death forward: the age of onset of cancers keeps getting younger.
As a defence against this oxidative attack, the liver produces an anti-oxidant called cholesterol.
Epidemiologically, the consumption of chlorinated water also produces a doubling of the rate of ischaemic heart failures from excess cholesterol, slightly in advance of the doubling of the incidence of carcinomas.
Lowering cholesterol by using drugs and restricting dietary cholesterol, as opposed to increasing the intake of antioxidants such as vitamin C (or getting off the chlorinated water supply), only changes the ratio between the rates of ischaemic heart failures and carcinomas, i.e. as heart failure rates go down due to medical intervention, the defence against cancers diminishes and cancer rates go up.
On average, the two epidemics of carcinomas and ischaemic heart failures each account for around one third of all deaths, i.e. on a chlorinated water supply a person has 2 chances in 3 of being killed by it.
These deaths are avoidable.
Regrettably this madness is enshrined in law and largely unopposed by those being killed by it.
Similarly, the practice of chlorination is largely unopposed by the medical industry with the result that the public health system is now grossly overloaded.
Here in New Zealand, the Government's Ministry of Health (sic) claims to use the "best and most up to date information available" and continues to mandate chlorination, in defiance of the EPA's advice.
And Housing, another monumental disaster mandated by law
High on the list of a Government's responsibilities must be the safeguarding of health and housing. Yet, like the heart failure and cancer epidemics, housing is another example of serious harm being caused by a regulatory/corporate scam that promises well-being and security but does nothing of the sort.
In New Zealand in the 1970s the corporates in the construction industry set out to limit the quality of housing, effectively to reduce the lifespan of houses to that of a consumer product rather than an asset that would last for generations.
That aim was achieved, in part, by reducing the structural bracing in houses by a half so that the remaining bracing was just enough to survive a "design earthquake" and no more.
In commercial design this lack of a safety factor is called the "ultimate loads" philosophy.
The "safety factor" in houses, it was decided, could be taken up by Gibraltar board (Gib).
However, bracing should behave in a "plastic" fashion by flexing under load then returning to its original shape after loads are removed. Gib is not bracing. It is stiffening; a rigid membrane that can only function once and then has to be replaced at considerable cost and inconvenience.
Since then Gib has taken over the "bracing" role entirely, in other words, houses are no longer braced at all. In the event of a 'quake greater than a design earthquake, a Gib "braced" house is damaged beyond repair and requires either demolition or substantial rebuild.
These houses built in New Zealand under the Building Act are a liability, not an asset, and home- owners are being duped.
For anyone able to consider home ownership, it may well be wise to consider a home built before the Building Act. The magic Certificate of Code Compliance may not be the guarantee one might hope for and, perhaps, the commonly used term "Coda Compliance" has an unintended warning of impending rebuilding.
We have been down this road before. The leaky housing fiasco was fed by two main factors, leaky flashings and untreated, non-durable radiata pine, both expected (and intended) to shorten the life of houses. The "problem" was that the reduction in longevity was more than expected and the media, nasty people, gave it "unnecessary" publicity.
The flashings used in leaky monolithic cladding systems are fitted against the wall framing, therefore are able to leak against that framing.
Today these leaky flashings are still being used for monolithic claddings and, in an effort to reduce longevity in other cladding types, are now mandatory for all claddings, including bevel back weatherboards which previously used flashings that did not leak.
New houses are being built in New Zealand under an Act of Parliament that purports to be protecting home owners but does not. What it does do is allow for regulations and rules that set a "minimum standard" so low as to not meet the performance requirements of the Act, and the people being protected are not the homeowners but the purveyors of the shonky products.
In effect the Act sets out a performance standard and the Regulations do the opposite. The Regulations are merely a tool used by business "stakeholders" to line their pockets with impunity.
Unfortunately, attempting to design or build to a better standard than minimum is almost guaranteed to be be met with push-back by local authorities, for reasons set out below.
The devil is in the detail
These serious burdens on society cannot be placed at the feet of any single political party. It would be difficult to criticise the intent of the various Acts of Parliament that create law to safeguard public health or to ensure that buildings are fit for purpose and so on.
However, while the principal Acts usually set out "performance standards" that are not prescriptive, those standards are then met by the secondary legislation or rules and regulations - and it is here that the law gets seriously hijacked.
For example, the Building Act requires that a building should not leak or be damp. That seems reasonable, so no problem there. But when we get down to the Regulations we that find there are two means of compliance: the "Acceptable Solution" or the "Alternative Solution."
The Acceptable Solution provides a "safe haven" for all parties: the local Council who issues the building consent is protected from litigation or any blame if things go wrong, likewise the building contractor is "blameless." Both parties are protected because the Acceptable Solution has been "deemed" to comply with the performance requirements of the Building Act, whether or not it does so in practice. Failed products are simply "deemed" to meet the performance standard.
This is manipulation of the worst sort. These parties are coerced, using fear tactics, into using the Acceptable Solutions rather than allowing skill, experience and common sense to be exercised.
The Regulations are formulated by a government department somewhere, in liason with key business interests or "stakeholders." These regulations become highly prescriptive and seriously restrict freedom of choice.
The regulations often lock in "product" that becomes the only means of compliance with the performance standard of the primary legislation, even if it monumentally fails to do so.
Because the purveyors of these shonky product are indemnified, when it all goes wrong it is the taxpayer who has to pick up the tab and there is no compensation for any victims who suffer harm.
The fine print in the Drinking Water Regulations
There should be two barriers to infection to meet the requirements of a safe drinking water supply.
The first barrier to infection is a clean water source. The second barrier is controlling contamination of the reticulation system.
Here in New Zealand we are a long narrow country with a good supply of pristine mountain water and there is no insurmountable difficulty obtaining water from these sources.
The second barrier to infection should be, taking the advice of the EPA, log3 point-of-use filtration. So a clean source and point-of-use filtration to 1 micron absolute satisfies the performance requirements of the primary legislation.
However, the regulators have set up a system for the grading of water supplies. Using that system, if a water supplier chlorinates then they will go straight to the top of the class with an A+ grading, regardless of any deficiencies in their water supply system and regardless of the harm chlorination causes.
Additionally, a water supplier's chances of obtaining funding assistance from Government go up.
In effect, this is manipulation of water suppliers by using a system of rewards and the fear of penalties on a bunch of people whose moral compass doesn't extend further than just wanting to clock off their 7 hour shift and go home.
Of course the chemical company, the "stakeholder" selling the chlorine, makes a sale and is indemnified by the legislation.
The fine print in Driver Licence Photos
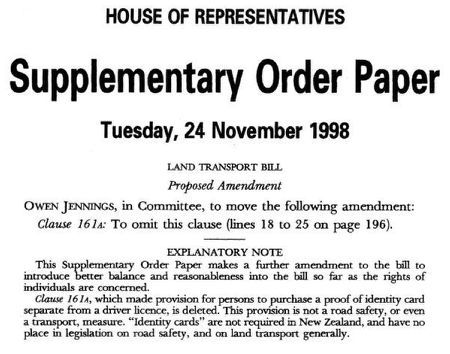
A further example, and one that gives more of a pointer to the underlying philosophy for these aberrations beyond a simple desire for business to make a quick buck, is the dastardly imposition of photo ID driver licences in New Zealand.
As the then New Zealand Privacy Commissioner, Bruce Slane, succinctly put it:

The Act creating the photographic driver licence was put to Parliament as a Bill that purported to improve road safety if the Police were able to view a person's licence with a photo on it at the roadside.
Of course there was no evidence presented to Parliament to support this claim and following the introduction of the photo licence the incidence of injury accidents went up significantly. This was only mitigated over the following decade by improvements in vehicle safety.
The Bill, it was claimed, allowed for an ordinary photograph, albeit a digital one, and was not to be amenable in any way for use by facial recognition algorithm. It was also claimed that there was no intention that such a licence would ever be used as an ID card.
In fact, Supplementary Order Paper 137 (SOP137) was tabled in the House to ensure that the driver licence, even with a photo on it, would not then become an ID card. A separate card would be required for ID for those wanting an ID card as proof of age for entry to pubs and other venues.
The ink had hardly dried when the Government introduced a further Bill related to a single prison escapee, a sex offender and murderer who was paroled and skipped the country on a passport in his birth name, issued by Internal Affairs, rather than the name he was imprisoned with.
The new Bill was an "omnibus" Bill that had the effect of changing other Acts. The laboriously named Enhancing Identity Verification und Border Processing Legislation Bill gave government departments access to the driver licence facial recognition (FR) photo database.
The Bill changed Section 200 of the Land Transport Act that had previously restricted access to the FR database in accordance with SOP 137.
Internal Affairs, in particular, were given carte blanch access to the database for any purpose at all, a sweeping power that pops up again with such initiatives as RealMe and, more recently, Identity Check.
But how did the photo database get to be FR and be vulnerable to subsequent abuses of this sort?
The initial prohibition on using the driver licence for FR was in the primary legislation as passed by Parliament. But middle management in the form of the NZTA (LTSA as it was then, or Waka Kotahi NZTA as it is now) had already committed itself to illegally doing the opposite by devious manipulation of the regulations.
The format of the driver licence was set out in two discussion papers put out by the NZTA. First came the Yellow Paper for public feedback. This was to be followed by consideration of public feedback and then a Green Draft that incorporated changes as a result of those considerations.
The Yellow Paper shed no light at all on the intended format of the new driver licence. It only set out the format for ID cards as required for the likes of bus drivers, taxi operators and so on. These ID cards were quite simple and didn't follow any recognised ID card format.
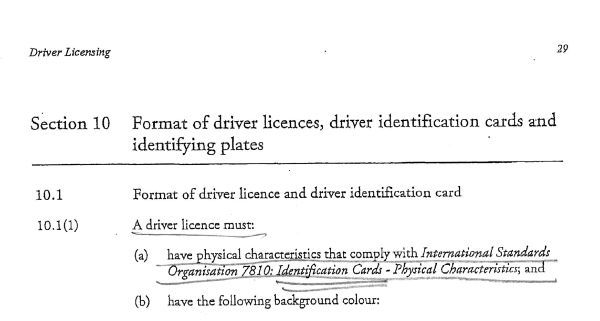
The subsequent Green Paper, not released for public comment, defined the driver licence as complying with international standards for ID cards, contrary to the limitations set out in the Bill.
The Green Paper only went to "stakeholders," an ominous word we will meet again, and there was no public consultation.
Part of this process necessarily involved a Privacy Impact Assessment (PIA).
The PIA was available at the time of the issue of the Yellow Draft but was not supplied to those who sought it until after the closing date for submissions. When submitters did finally receive the PIA they found that it was based on the driver licence format very clearly set out in the later Green draft.
For the PIA to be complete at the time of issue of the Yellow draft, the Green draft on which the PIA was based must also have been in existence.
In other words, the truth was withheld from the public. The middle management snakes-in-the-grass had already done a deal with industry players to make the driver licence a vehicle for an ID card, and a facial recognition one at that.
Simply put, there was only one paper, the Green Paper. The Yellow Paper was a hoax.
Existing "lifetime" licences were all expired within 12 months, of course. Like many contracts with government, they were simply not honoured.
Clearly, coercion played a significant role in this process.
Is the NZ Driver Licence a driver licence or an ID card?
I add this new section for clarity because feedback suggests that most people do not perceive the NZ driver licence as an ID card except that it is amenable to being used as such. This is not correct.
The Green Paper clearly set out that the driver licence would conform to the International Standard 7810 for ID cards.
The decision to make the driver licence an ID card was made before the decision of the House to amend the Act to ensure that it could not be an ID card.
The Privacy Commissioner, Bruce Slane, was certainly on to the connection between the driver licence and the ID card but was not privy to sufficient information to realize that his cartoon was back to front: in fact, the driver licence information was tacked on to an ID card, not the other way around.
The decision to implement an ID card was made around or before November 1997. The amendment of the Act to make this illegal was made around the end of 1998.
But LTSA had already entered contracts, etc, etc so the ID card came into being and nobody had the backbone to call it for what it was.
Finger prints and Face prints
Further, recognising the driver licence more correctly as an ID card raises another privacy issue.
If a person falls foul of the criminal system then they will have their fingerprints taken. Fingerprints are not an ordinary photo of a person's hand but a more detailed image of the markings on the hand that enables police to distinguish one hand from many.
If a person obtains a driver licence, aka, an ID card from Waka Kotahi NZTA then they will have a face image taken that has sufficient detail to enable that one face image to be distinguished from many face images.
In the very hard to obtain Privacy Impact Assessment of 1997, Part 2 Storage of Digitised Image, LTSA Analysis, Necessity for Image Storage, paragraph 3, the LTSA stated "While this is new technology in terms of driver licensing in New Zealand, it is similar to that commonly used for fingerprint matching."
So there it is from the horse's mouth, the NZ driver licence photo is actually an alternative to fingerprints.
With increasing demands to provide ID for everyday transactions comes the increasing necessity to rely on a fingerprint or a face print on a daily basis.
In effect New Zealand has become a prison where almost all residents carry around digital forms of fingerprint or face print to prove identity, absolutely illegally, as contrived by government departments and their ad hoc business units - while democratic process and Parliament have become little more than childish theatrics.
No car? No photo ID? Then you need a National Ticketing Solution
The National Ticketing Solution (NTS) requires that anyone using public transport must use a card, either a physical card (for those without an iPhone and under a certain age) or an "app" (all adults).
This is a pass card not unlike the photographic driver licence and, together, these mean that any form of movement within New Zealand will require a defacto passport. Both will have a facial recognition component.
Such a draconian and fundamental change to our rights and freedoms didn't occur through the introduction of a new Bill to that effect, didn't involve any public consultation at all and didn't involve any debate in the House of Parliament.
Like a thief, it crept in through the back door as fine print in the Land Transport (NZTA) Legislation Amendment Bill.
That Bill was also an Omnibus Bill. Provisions in the Bill amended the existing Land Transport Management Act 2003 by including a new part (o) in Section 95 Functions of Agency (1):
"(o) to deliver, or manage the delivery of, activities for ticketing systems and payments in relation to the land transport system (and for this purpose, the statutory exemption in section 43 of the Commerce Act 1986 applies to any activities delivered or managed in accordance with this provision)"
The purpose of the Commerce Act is "to promote competition in markets for the long-term benefit of consumers within New Zealand." Being exempt from provisions of this Act gives the NZTA the legal right to act, or incite others to act on its behalf, as a cartel, essentially above the law.
The Bill went through all readings in the House bar the third reading. Until then there was no hint of giving such draconian powers to the NZTA.
But a Supplementary Order Paper no.546 (SOP546) was tabled on Tuesday 21st July 2020 and contained the above amendment to (o).
The prior Disclosure Statement relating to the first reading of the Bill did not cover this monumental change, of course.
The next day, Wednesday 22nd, the third and final reading containing the SOP passed without debate, without dissent, without public disclosure or feedback, in short it was a travesty of democracy and justice.
Since then the NZTA has produced the National Ticketing Solution (the NTS).
This is an "open" system. The currently used Snapper card is a "closed" system meaning the card is reloaded from time to time, whereas the NTS "open" system gives the NZTA or its agent the right to keep a record of a card holder's movements during the day, i.e. track the movements of the holder, and then bill their bank account overnight.
Currently Snapper is used and cash is accepted. It is highly unlikely cash will be accepted once the NTS is up and running. Photographic ID will be required to onboard the NTS, most likely at the banking end of the system.
A Privacy Impact Assessment is planned. After contracts with suppliers are locked in place and the system is up and running. Of course.
"Stakeholders"
In a world where it seems everyone has some sort of agenda, there is a thread that is common to much of what happens in these abuses of Parliamentary process and that is the mantra of a government and stakeholder partnership.
This philosophy, and it is a religion bordering on a cult, says that the world will be a better place if business takes the place of voters in the democratic system. It argues that prosperity will result and we will all be better off and more content, if we are prepared to forgo our free will.
This shallow philosophy, that goes no deeper than material advancement over all else, has many adherents. The list is long. Presidents, Prime Ministers, influential politicians, bankers - if you ever thought that "so and so" was trying to rule the world, think again. You'll probably find he or she is merely part of the "club."
Discussion
In my opinion the evidence points to the deliberate betrayal of our democratic system. The consistency of the methods used to undermine Parliamentary process and hijack our way of life demonstrates a careful and manipulative approach to creating the sorts of harm outlined above.
These methods go well beyond self interest by a few over zealous businessmen.
One could be forgiven for thinking that there is a whole department of behavioural psychologists beavering away somewhere whose sole task is to find new ways of manipulating society into destroying itself.
The obvious is, surely, that if something is good for us then it will stand on its own merits. It should not require devious and underhand methods to get it over the line.
The erosion of our right to exercise free will suggests that behind the scenes is the planned end of democracy and the locking in of another fascist era beyond which, short of a miracle, there is little hope if we do not take back ownership of our system of open and accountable governance while we can.
As a start that should require a clear acknowledgement by Government that crucial legislation has not been created by lawful process. Unless there is acknowledgement that human rights have been compromised as a result then it seems to me there is little hope of taking action to put things right.
January 21, 2023
Amended March 4, 2023
In 2003, the United States Environmental Protection Agency (EPA) declared that the link between the chlorination of drinking water and cancer was sufficient to require regulatory action to retire chlorination and replace it with filtration.
The EPA stated:
" III Public Health Risk
Chlorine has been widely used as a chemical disinfectant, serving as a principal barrier to microbial contaminants in drinking water. However, the microbial risk reduction attributes of chlorination have been increasingly scrutinized due to concerns about potential increased health risks ... new health studies continue to support an association between bladder, colon and rectal cancers from long-term exposure to chlorinated surface water. In addition to cancer effects, recent studies have reported associations between use of chlorinated drinking water and a number of reproductive and developmental endpoints including spontaneous abortion, still birth, neural tube defect, pre-term delivery, low birth weight and intrauterine growth retardation (small for gestational age)...Based on the weight of evidence from both the human epidemiology and animal toxicology data on cancer and reproductive and developmental health effects and consideration of the large number of people exposed ... the combined health data warrant regulatory action..." ( Federal Register / Vol.68. No. 159 / Monday, August 18, 2003 / Proposed Rules p. 49557 )
A brief summary of the Cancer and Heart Failure Epidemics
Epidemiologically, the cancer rate doubles in the first 12 months following the start of chlorination of any particular drinking water supply.
Those who die in the first 12 months are mainly in the 70+ age bracket.
Chlorine gas used to treat drinking water produces hypochlorous acid and it is this strong oxidising agent that acts as the disinfectant.
Hypochlorous acid is not selective. As well as oxidising bacteria and killing them, it oxidises human cells causing damage leading to mutation and cancer.
Over the course of a lifetime the consumption of hypochlorous acid in chlorinated water moves the age of cancer initiated death forward: the age of onset of cancers keeps getting younger.
As a defence against this oxidative attack, the liver produces an anti-oxidant called cholesterol.
Epidemiologically, the consumption of chlorinated water also produces a doubling of the rate of ischaemic heart failures from excess cholesterol, slightly in advance of the doubling of the incidence of carcinomas.
Lowering cholesterol by using drugs and restricting dietary cholesterol, as opposed to increasing the intake of antioxidants such as vitamin C (or getting off the chlorinated water supply), only changes the ratio between the rates of ischaemic heart failures and carcinomas, i.e. as heart failure rates go down due to medical intervention, the defence against cancers diminishes and cancer rates go up.
On average, the two epidemics of carcinomas and ischaemic heart failures each account for around one third of all deaths, i.e. on a chlorinated water supply a person has 2 chances in 3 of being killed by it.
These deaths are avoidable.
Regrettably this madness is enshrined in law and largely unopposed by those being killed by it.
Similarly, the practice of chlorination is largely unopposed by the medical industry with the result that the public health system is now grossly overloaded.
Here in New Zealand, the Government's Ministry of Health (sic) claims to use the "best and most up to date information available" and continues to mandate chlorination, in defiance of the EPA's advice.
And Housing, another monumental disaster mandated by law
High on the list of a Government's responsibilities must be the safeguarding of health and housing. Yet, like the heart failure and cancer epidemics, housing is another example of serious harm being caused by a regulatory/corporate scam that promises well-being and security but does nothing of the sort.
In New Zealand in the 1970s the corporates in the construction industry set out to limit the quality of housing, effectively to reduce the lifespan of houses to that of a consumer product rather than an asset that would last for generations.
That aim was achieved, in part, by reducing the structural bracing in houses by a half so that the remaining bracing was just enough to survive a "design earthquake" and no more.
In commercial design this lack of a safety factor is called the "ultimate loads" philosophy.
The "safety factor" in houses, it was decided, could be taken up by Gibraltar board (Gib).
However, bracing should behave in a "plastic" fashion by flexing under load then returning to its original shape after loads are removed. Gib is not bracing. It is stiffening; a rigid membrane that can only function once and then has to be replaced at considerable cost and inconvenience.
Since then Gib has taken over the "bracing" role entirely, in other words, houses are no longer braced at all. In the event of a 'quake greater than a design earthquake, a Gib "braced" house is damaged beyond repair and requires either demolition or substantial rebuild.
These houses built in New Zealand under the Building Act are a liability, not an asset, and home- owners are being duped.
For anyone able to consider home ownership, it may well be wise to consider a home built before the Building Act. The magic Certificate of Code Compliance may not be the guarantee one might hope for and, perhaps, the commonly used term "Coda Compliance" has an unintended warning of impending rebuilding.
We have been down this road before. The leaky housing fiasco was fed by two main factors, leaky flashings and untreated, non-durable radiata pine, both expected (and intended) to shorten the life of houses. The "problem" was that the reduction in longevity was more than expected and the media, nasty people, gave it "unnecessary" publicity.
The flashings used in leaky monolithic cladding systems are fitted against the wall framing, therefore are able to leak against that framing.
Today these leaky flashings are still being used for monolithic claddings and, in an effort to reduce longevity in other cladding types, are now mandatory for all claddings, including bevel back weatherboards which previously used flashings that did not leak.
New houses are being built in New Zealand under an Act of Parliament that purports to be protecting home owners but does not. What it does do is allow for regulations and rules that set a "minimum standard" so low as to not meet the performance requirements of the Act, and the people being protected are not the homeowners but the purveyors of the shonky products.
In effect the Act sets out a performance standard and the Regulations do the opposite. The Regulations are merely a tool used by business "stakeholders" to line their pockets with impunity.
Unfortunately, attempting to design or build to a better standard than minimum is almost guaranteed to be be met with push-back by local authorities, for reasons set out below.
The devil is in the detail
These serious burdens on society cannot be placed at the feet of any single political party. It would be difficult to criticise the intent of the various Acts of Parliament that create law to safeguard public health or to ensure that buildings are fit for purpose and so on.
However, while the principal Acts usually set out "performance standards" that are not prescriptive, those standards are then met by the secondary legislation or rules and regulations - and it is here that the law gets seriously hijacked.
For example, the Building Act requires that a building should not leak or be damp. That seems reasonable, so no problem there. But when we get down to the Regulations we that find there are two means of compliance: the "Acceptable Solution" or the "Alternative Solution."
The Acceptable Solution provides a "safe haven" for all parties: the local Council who issues the building consent is protected from litigation or any blame if things go wrong, likewise the building contractor is "blameless." Both parties are protected because the Acceptable Solution has been "deemed" to comply with the performance requirements of the Building Act, whether or not it does so in practice. Failed products are simply "deemed" to meet the performance standard.
This is manipulation of the worst sort. These parties are coerced, using fear tactics, into using the Acceptable Solutions rather than allowing skill, experience and common sense to be exercised.
The Regulations are formulated by a government department somewhere, in liason with key business interests or "stakeholders." These regulations become highly prescriptive and seriously restrict freedom of choice.
The regulations often lock in "product" that becomes the only means of compliance with the performance standard of the primary legislation, even if it monumentally fails to do so.
Because the purveyors of these shonky product are indemnified, when it all goes wrong it is the taxpayer who has to pick up the tab and there is no compensation for any victims who suffer harm.
The fine print in the Drinking Water Regulations
There should be two barriers to infection to meet the requirements of a safe drinking water supply.
The first barrier to infection is a clean water source. The second barrier is controlling contamination of the reticulation system.
Here in New Zealand we are a long narrow country with a good supply of pristine mountain water and there is no insurmountable difficulty obtaining water from these sources.
The second barrier to infection should be, taking the advice of the EPA, log3 point-of-use filtration. So a clean source and point-of-use filtration to 1 micron absolute satisfies the performance requirements of the primary legislation.
However, the regulators have set up a system for the grading of water supplies. Using that system, if a water supplier chlorinates then they will go straight to the top of the class with an A+ grading, regardless of any deficiencies in their water supply system and regardless of the harm chlorination causes.
Additionally, a water supplier's chances of obtaining funding assistance from Government go up.
In effect, this is manipulation of water suppliers by using a system of rewards and the fear of penalties on a bunch of people whose moral compass doesn't extend further than just wanting to clock off their 7 hour shift and go home.
Of course the chemical company, the "stakeholder" selling the chlorine, makes a sale and is indemnified by the legislation.
The fine print in Driver Licence Photos
A further example, and one that gives more of a pointer to the underlying philosophy for these aberrations beyond a simple desire for business to make a quick buck, is the dastardly imposition of photo ID driver licences in New Zealand.
As the then New Zealand Privacy Commissioner, Bruce Slane, succinctly put it:
The Act creating the photographic driver licence was put to Parliament as a Bill that purported to improve road safety if the Police were able to view a person's licence with a photo on it at the roadside.
Of course there was no evidence presented to Parliament to support this claim and following the introduction of the photo licence the incidence of injury accidents went up significantly. This was only mitigated over the following decade by improvements in vehicle safety.
The Bill, it was claimed, allowed for an ordinary photograph, albeit a digital one, and was not to be amenable in any way for use by facial recognition algorithm. It was also claimed that there was no intention that such a licence would ever be used as an ID card.
In fact, Supplementary Order Paper 137 (SOP137) was tabled in the House to ensure that the driver licence, even with a photo on it, would not then become an ID card. A separate card would be required for ID for those wanting an ID card as proof of age for entry to pubs and other venues.
The ink had hardly dried when the Government introduced a further Bill related to a single prison escapee, a sex offender and murderer who was paroled and skipped the country on a passport in his birth name, issued by Internal Affairs, rather than the name he was imprisoned with.
The new Bill was an "omnibus" Bill that had the effect of changing other Acts. The laboriously named Enhancing Identity Verification und Border Processing Legislation Bill gave government departments access to the driver licence facial recognition (FR) photo database.
The Bill changed Section 200 of the Land Transport Act that had previously restricted access to the FR database in accordance with SOP 137.
Internal Affairs, in particular, were given carte blanch access to the database for any purpose at all, a sweeping power that pops up again with such initiatives as RealMe and, more recently, Identity Check.
But how did the photo database get to be FR and be vulnerable to subsequent abuses of this sort?
The initial prohibition on using the driver licence for FR was in the primary legislation as passed by Parliament. But middle management in the form of the NZTA (LTSA as it was then, or Waka Kotahi NZTA as it is now) had already committed itself to illegally doing the opposite by devious manipulation of the regulations.
The format of the driver licence was set out in two discussion papers put out by the NZTA. First came the Yellow Paper for public feedback. This was to be followed by consideration of public feedback and then a Green Draft that incorporated changes as a result of those considerations.
The Yellow Paper shed no light at all on the intended format of the new driver licence. It only set out the format for ID cards as required for the likes of bus drivers, taxi operators and so on. These ID cards were quite simple and didn't follow any recognised ID card format.
The subsequent Green Paper, not released for public comment, defined the driver licence as complying with international standards for ID cards, contrary to the limitations set out in the Bill.
The Green Paper only went to "stakeholders," an ominous word we will meet again, and there was no public consultation.
Part of this process necessarily involved a Privacy Impact Assessment (PIA).
The PIA was available at the time of the issue of the Yellow Draft but was not supplied to those who sought it until after the closing date for submissions. When submitters did finally receive the PIA they found that it was based on the driver licence format very clearly set out in the later Green draft.
For the PIA to be complete at the time of issue of the Yellow draft, the Green draft on which the PIA was based must also have been in existence.
In other words, the truth was withheld from the public. The middle management snakes-in-the-grass had already done a deal with industry players to make the driver licence a vehicle for an ID card, and a facial recognition one at that.
Simply put, there was only one paper, the Green Paper. The Yellow Paper was a hoax.
Existing "lifetime" licences were all expired within 12 months, of course. Like many contracts with government, they were simply not honoured.
Clearly, coercion played a significant role in this process.
Is the NZ Driver Licence a driver licence or an ID card?
I add this new section for clarity because feedback suggests that most people do not perceive the NZ driver licence as an ID card except that it is amenable to being used as such. This is not correct.
The Green Paper clearly set out that the driver licence would conform to the International Standard 7810 for ID cards.
The decision to make the driver licence an ID card was made before the decision of the House to amend the Act to ensure that it could not be an ID card.
The Privacy Commissioner, Bruce Slane, was certainly on to the connection between the driver licence and the ID card but was not privy to sufficient information to realize that his cartoon was back to front: in fact, the driver licence information was tacked on to an ID card, not the other way around.
The decision to implement an ID card was made around or before November 1997. The amendment of the Act to make this illegal was made around the end of 1998.
But LTSA had already entered contracts, etc, etc so the ID card came into being and nobody had the backbone to call it for what it was.
Finger prints and Face prints
Further, recognising the driver licence more correctly as an ID card raises another privacy issue.
If a person falls foul of the criminal system then they will have their fingerprints taken. Fingerprints are not an ordinary photo of a person's hand but a more detailed image of the markings on the hand that enables police to distinguish one hand from many.
If a person obtains a driver licence, aka, an ID card from Waka Kotahi NZTA then they will have a face image taken that has sufficient detail to enable that one face image to be distinguished from many face images.
In the very hard to obtain Privacy Impact Assessment of 1997, Part 2 Storage of Digitised Image, LTSA Analysis, Necessity for Image Storage, paragraph 3, the LTSA stated "While this is new technology in terms of driver licensing in New Zealand, it is similar to that commonly used for fingerprint matching."
So there it is from the horse's mouth, the NZ driver licence photo is actually an alternative to fingerprints.
With increasing demands to provide ID for everyday transactions comes the increasing necessity to rely on a fingerprint or a face print on a daily basis.
In effect New Zealand has become a prison where almost all residents carry around digital forms of fingerprint or face print to prove identity, absolutely illegally, as contrived by government departments and their ad hoc business units - while democratic process and Parliament have become little more than childish theatrics.
No car? No photo ID? Then you need a National Ticketing Solution
The National Ticketing Solution (NTS) requires that anyone using public transport must use a card, either a physical card (for those without an iPhone and under a certain age) or an "app" (all adults).
This is a pass card not unlike the photographic driver licence and, together, these mean that any form of movement within New Zealand will require a defacto passport. Both will have a facial recognition component.
Such a draconian and fundamental change to our rights and freedoms didn't occur through the introduction of a new Bill to that effect, didn't involve any public consultation at all and didn't involve any debate in the House of Parliament.
Like a thief, it crept in through the back door as fine print in the Land Transport (NZTA) Legislation Amendment Bill.
That Bill was also an Omnibus Bill. Provisions in the Bill amended the existing Land Transport Management Act 2003 by including a new part (o) in Section 95 Functions of Agency (1):
"(o) to deliver, or manage the delivery of, activities for ticketing systems and payments in relation to the land transport system (and for this purpose, the statutory exemption in section 43 of the Commerce Act 1986 applies to any activities delivered or managed in accordance with this provision)"
The purpose of the Commerce Act is "to promote competition in markets for the long-term benefit of consumers within New Zealand." Being exempt from provisions of this Act gives the NZTA the legal right to act, or incite others to act on its behalf, as a cartel, essentially above the law.
The Bill went through all readings in the House bar the third reading. Until then there was no hint of giving such draconian powers to the NZTA.
But a Supplementary Order Paper no.546 (SOP546) was tabled on Tuesday 21st July 2020 and contained the above amendment to (o).
The prior Disclosure Statement relating to the first reading of the Bill did not cover this monumental change, of course.
The next day, Wednesday 22nd, the third and final reading containing the SOP passed without debate, without dissent, without public disclosure or feedback, in short it was a travesty of democracy and justice.
Since then the NZTA has produced the National Ticketing Solution (the NTS).
This is an "open" system. The currently used Snapper card is a "closed" system meaning the card is reloaded from time to time, whereas the NTS "open" system gives the NZTA or its agent the right to keep a record of a card holder's movements during the day, i.e. track the movements of the holder, and then bill their bank account overnight.
Currently Snapper is used and cash is accepted. It is highly unlikely cash will be accepted once the NTS is up and running. Photographic ID will be required to onboard the NTS, most likely at the banking end of the system.
A Privacy Impact Assessment is planned. After contracts with suppliers are locked in place and the system is up and running. Of course.
"Stakeholders"
In a world where it seems everyone has some sort of agenda, there is a thread that is common to much of what happens in these abuses of Parliamentary process and that is the mantra of a government and stakeholder partnership.
This philosophy, and it is a religion bordering on a cult, says that the world will be a better place if business takes the place of voters in the democratic system. It argues that prosperity will result and we will all be better off and more content, if we are prepared to forgo our free will.
This shallow philosophy, that goes no deeper than material advancement over all else, has many adherents. The list is long. Presidents, Prime Ministers, influential politicians, bankers - if you ever thought that "so and so" was trying to rule the world, think again. You'll probably find he or she is merely part of the "club."
Discussion
In my opinion the evidence points to the deliberate betrayal of our democratic system. The consistency of the methods used to undermine Parliamentary process and hijack our way of life demonstrates a careful and manipulative approach to creating the sorts of harm outlined above.
These methods go well beyond self interest by a few over zealous businessmen.
One could be forgiven for thinking that there is a whole department of behavioural psychologists beavering away somewhere whose sole task is to find new ways of manipulating society into destroying itself.
The obvious is, surely, that if something is good for us then it will stand on its own merits. It should not require devious and underhand methods to get it over the line.
The erosion of our right to exercise free will suggests that behind the scenes is the planned end of democracy and the locking in of another fascist era beyond which, short of a miracle, there is little hope if we do not take back ownership of our system of open and accountable governance while we can.
As a start that should require a clear acknowledgement by Government that crucial legislation has not been created by lawful process. Unless there is acknowledgement that human rights have been compromised as a result then it seems to me there is little hope of taking action to put things right.
January 21, 2023
Amended March 4, 2023
Index (under construction) wairarapa.health@yahoo.com
mandatory bad building practices
666 or 616?
a Simple Guide to the Far Right
religious objection to Facial Recognition