Tap water pH adjustment and heart disease.
The connection between chlorinated drinking water and cholesterol has been known for some time. Much research has been done on that connection, and in 1985 the Environmental Protection Agency (EPA) in the United States helped to fund research at the Oak Ridge Research Institute to test the validity of previous research on this subject.
The logical conclusion of the EPA funded research is that water pH, cholesterol and chlorine are interactive factors in the association between chlorine and heart failure.
This case study looks at one of those factors, water pH. The other factors will be found elsewhere in www.cancer.net.nz in due course, so I won't duplicate that material here.
Research by Oak Ridge Research Institute and the EPA
The use of chlorine as a disinfectant of public drinking water supplies was first practiced in the United States in 1908 (1). The benefit of chlorine on controlling levels of water-borne infectious bacteria soon became known, and the practice of chlorination spread to most large population centers within a decade. The EPA office of water supply estimates that in 1975, 192 million Americans were served by community water systems, and the majority of these systems used chlorine as a disinfectant (2). Other disinfectants used in drinking water systems include chlorine dioxide, monochloramine, and ozone.
The health benefits associated with chlorination are well established, but the possibility of harmful effects also exists. For instance, recent studies suggest that hepatotoxins and carcinogens may be generated during chlorination (3, 4). The compounds generated include chlorinated organics such as chloroform and other trihalomethanes, both of which have been observed in drinking water treated with chlorine (5). Chlorination of foods and drinking water have been associated with cardiovascular abnormalities. For example, the chlorination of flour is associated with the formation of chlorinated fatty acids, and, in animals fed these fatty acids, significant increases in heart weight have been observed (6). Revis et al. (7) have observed hypercholesterolemia and cardiac hypertrophy in pigeons and rabbits exposed to chlorinated drinking water. Taken together, these results suggest that chlorine and/or formed chlorinated products may adversely affect the cardiovascular system through the well-known association of plasma cholesterol levels with atherosclerosis and hypertension with cardiac hypertrophy.
To further explore the possible relationship of drinking water disinfectants to cardiovascular disease, pigeons were exposed to drinking water containing different concentrations of chlorine, chlorine dioxide, and monochloramine. The effect of these disinfectants on the cardiovascular system was determined by measuring plasma cholesterol and the presence and severity of coronary and aortic atherosclerosis. Thyroid function was determined because in previous studies we have observed a significant decrease in plasma thyroxine (T4) in pigeons treated with chlorinated drinking water. These studies were performed also because of the known association between cardiac hypertrophy and hypercholesterolemia with plasma thyroid hormone levels (8, 9).
The following is part of the 1985 research (the full version can be googled);
Relationship of drinking water disinfectants to plasma cholesterol
and thyroid hormone levels in experimental studies.
Proc. Natl. Acad. Sci. USA
Vol. 83, pp. 1485-1489, March 1986
Medical Sciences
N. W. REVIS1,2, P. MCCAULEY2, R. BULL2, AND G. HOLDSWORTH1
1Oak Ridge Research Institute, 113 Union Valley Road, Oak Ridge, TN 37830; and
2United States Environmental Protection Agency, 26 West St. Clair Street, Cincinnati, Ohio 45219
Communicated by William A. Arnold, October 30, 1985
ABSTRACT The effects of drinking water containing 2 or 15 ppm chlorine (pH 6.5 and 8.5), chlorine dioxide, and monochloramine on thyroid function and plasma cholesterol were studied because previous investigators have reported cardiovascular abnormalities in experimental animals exposed to chlorinated water. Plasma thyroxine (T4) levels, as compared to controls, were significantly decreased in pigeons fed a normal or high-cholesterol diet and drinking water containing these drinking water disinfectants at a concentration of 15 ppm (the exception was chlorine at pH 6.5) for 3 months. In most of the treatment groups, T4 levels were significantly lower following the exposure to drinking water containing the 2 ppm dose. Increases in plasma cholesterol were frequently observed in the groups with lower T4 levels. This association was most evident in pigeons fed the high-cholesterol diet and exposed to these disinfectants at a dose of 15 ppm. For example, after 3 months of exposure to deionized water or water containing 15 ppm monochloramine, plasma cholesterol was 1266 � 172 and 2049 � 212 mg/dl, respectively, a difference of 783 mg/dl. The factor(s) associated with the effect of these disinfectants on plasma T4 and cholesterol is not known. We suggest however that these effects are probably mediated by products formed when these disinfectants react with organic matter in the upper gastrointestinal tract.
(BACKGROUND)
METHODS
Male white carneau pigeons (age, 3-4 months; obtained from Palmetto Pigeon Plant, Sumter, SC) were observed for 20 days prior to treatment. The effect of chlorine, chlorine dioxide, and monochloramine on the cardiovascular system was determined by exposing groups of 12 pigeons to drinking water containing these disinfectants and various pigeon diets for 3 months. The pigeon diets were prepared by Ralston Purina (St. Louis, MO) and altered from the normal pigeon diet as follows: diet A, reduction in calcium to 0.35% (80% of the minimum daily requirement for pigeons); diet B, reduction in calcium to 0.35% and the addition of 10% lard and 0.5% cholesterol. The concentrations of cholesterol in diet A over the experimental period ranged from 0.06% to 0.09%. Animals were exposed to the diets and drinking water ad lib. The drinking water contained chlorine, chlorine dioxide, and monochloramine at concentrations of 2 and 15 ppm. These disinfectants were prepared daily as described (10, 11). The drinking water was changed daily, and the level of each disinfectant and the pH were measured daily and adjusted (if required) to the level and pH indicated below. The controls were given deionized drinking water (or chlorite as a control to chlorine dioxide), which was changed daily.
RESULTS
In both control and experiment groups receiving the normal diet, plasma cholesterol increased from zero time to 3 months (Fig. LA). In the controls, plasma cholesterol was increased by 35 mg/dl at 3 months. In contrast, the mean increase in plasma cholesterol averaged 64 mg/dl in pigeons given the various drinking water disinfectants for 3 months. The range of increase over the controls in these various groups was from 5 to 173 mg/dl. However, significant increases in plasma cholesterol after 3 months of exposure were only observed in pigeons given chlorine at pH 8.5 (2 and 15 ppm), chlorine dioxide (2 ppm), and monochloramine (2 ppm). Although plasma cholesterol was increased in pigeons exposed to chlorite, the increase was not statistically significant because of the relatively large standard deviation. In none of the treatment groups was a clear dose-response effect for plasma cholesterol observed.
The mean average increases in plasma cholesterol in all groups exposed to the high-cholesterol diet (Fig. 1B) were from 168 + 8 (0 time) to 1505 � 215 (at 3 months). The 3-month value represents an =9-fold increase in plasma cholesterol in 90 days. Although increases compared to controls were observed in pigeons given 2 ppm chlorine (pH 6.5 and 8.5), significant increases at 3 months were only observed in pigeons given 15 ppm chlorine (pH 8.5), chlorine dioxide, and monochloramine. After 3 months of exposure to deionized water or 15 ppm monochloramine, the mean plasma cholesterol was 1266 + 172 and 2049 � 212, respectively - a difference of 783 cholesterol mg/dl. The range of increase over the controls in pigeons given the various drinking water disinfectants at 15 ppm was from 42 to 738 (sic) mg/dl. Although a dose-response effect was not observed, results suggest that the 15 ppm dose was more effective in increasing plasma cholesterol than was the 2 ppm dose.
DISCUSSION
Significant increases in plasma cholesterol were observed in pigeons given the various drinking water disinfectants. However, a clear dose-response effect was not observed, although pigeons were more responsive when given the 15-ppm dose and the high cholesterol diet or 2 ppm and the normal diet. In pigeons fed the normal diet, chlorine (pH 8.5) and chlorine dioxide (2 ppm) were both effective in the induction of an increase in plasma cholesterol, whereas in the high cholesterol diet studies, three disinfectants [i.e., 15 ppm chlorine (pH 8.5), chlorine dioxide, and monochloramine] were associated with significant increases in plasma cholesterol. Pigeons fed the two diets and exposed to chlorine (pH 6.5) showed insignificant increases in plasma cholesterol. Since the pH of the solutions containing chlorine, chlorine dioxide, and monochloramine ranged from 7.6 to 8.5, this suggests a relationship between pH, disinfectant dose, and plasma cholesterol. In previous studies we have not observed significant changes in plasma cholesterol in pigeons exposed to deionized water buffered to pHs of 7.0, 7.5, 8.5, and 9.5. This suggests that it is the disinfectant itself rather than the pH of the drinking water that is responsible for the observed plasma cholesterol effect.
We have observed significant increases in plasma cholesterol and aortic athero-sclerosis in pigeons exposed to three commonly used drinking water disinfectants. The atherosclerotic effects observed in these studies are probably related to increases in plasma cholesterol.
From this we can see that the currently accepted practice of adjusting pH after adding residual chlorine can be expected to increase heart failure. I am assuming that the pH of 6.5 is a result of adding chlorine disinfectant which makes the water acid and that the pH of 8.5 is a result of adding lime to the disinfected water.
In my previous case study of conductive water pipe in the North Island of New Zealand I controlled for pH by including only those results for water supplies in the pH range 7.5 - 8.5. That, of course, included nearly every water supply. There was an exception, however, and that was Taupo's water supply which doesn't have pH adjustment after chlorination. The system used is simply to filter and chlorinate.
The anomaly is that heart failure appeared to be lower than would be expected for the water treatment system being used, which suggested at the time that the connection between pH adjustment and heart failure was more complex than simply relating increased acidity to increased heart failure
Taupo case study
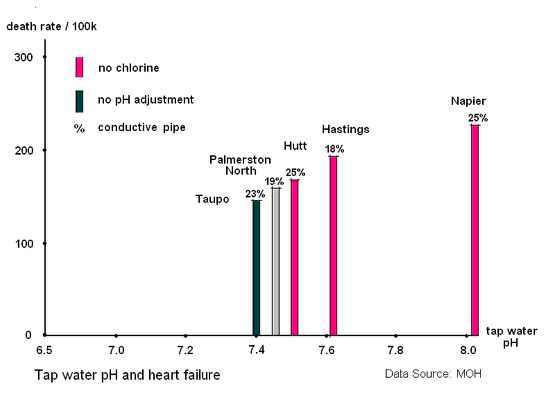
In any case, the purpose of this study is to compare the rate of heart failure in Taupo compared to water supplies generally to see if this comparison is consistent with the result from the EPA report. I have controlled for conductive pipe by working within +/- 5% of Taupo's amount of conductive pipe. Here's how it looks when graphed:
As can be seen, Taupo's heart failure rate is lower compared to other North Island towns with higher (more alkaline) water pHs, and is entirely consistent with the EPA report. The difference in deaths from heart failure for pHs between 7.4 and 8.2 is around 50% in this study compared to cholesterol increases of around 20% in the EPA study (despite the smaller pH range of this study), and is probably due to the EPA study being limited to 3 months.
Conclusion
Adjusting for pH, i.e. making drinking water less acid, has the opposite effect to that which might be expected: heart failure rates increase with alkalinity. This appears to elevate deaths from heart disease by about 50%, although the effect of dropping below a pH of 7.4 is not tested.
Given that distilled water is naturally slightly acid because it absorbs carbon dioxide, then it would not be unreasonable to say that water at a pH of 6.5 is not that different. The implication is that where residual chlorine is used, the pH should be kept slightly acid of 7.0 to mitigate heart disease and the currently accepted practice of adding lime to counteract residual chlorine appears to significantly contribute to the heart disease epidemic. Obviously the better solution is not to add the chlorine in the first place, given the likely implications for cancer rate changes.
Stephen G. Butcher (Posted 01/01/09)