Welcome to
cancer.net.nz
-keeping you informed with totally independent cancer research-
cancer.net.nz
-keeping you informed with totally independent cancer research-
Will I get cancer where I live?
For instance, the State of Israel has no escalating cancer epidemic, yet there are increases in incidence where groups emigrate from Russia or France to escape religious persecution. Once these groups are in Israel their incidence of cancer drops within 12 months.
Similarly, within cancer epidemic countries there is a wide variation in cancer registration rates between different towns and cities, and a person's risk of cancer is determined by the water supply of the area in which they live. For example, here in New Zealand cancer risk varies greatly between territorial land authorities (TLAs) as the following chart demonstrates:
Similarly, within cancer epidemic countries there is a wide variation in cancer registration rates between different towns and cities, and a person's risk of cancer is determined by the water supply of the area in which they live. For example, here in New Zealand cancer risk varies greatly between territorial land authorities (TLAs) as the following chart demonstrates:
Water naturally contains hydrogen ions called hydronium but these occur in very, very small amounts and are extremely short lived. However, the number of these hydronium ions can be greatly increased by the addition of chlorine. A similar effect occurs by forcing the pH to the alkaline side of neutral either by adding lime or sourcing water which hasn't had sufficient contact time with air. Chlorine added to water, for instance, produces hydrochloric acid which dissociates to form hydrogen ions as an acid condition, while lime has a similar effect in producing hydronium ions on the alkaline side.
Water chlorination was increased around 1991 to control an outbreak of cholera which was rapidly spreading through South America. Both heart failure and cancer death rates went up immediately, but the effect on heart failures is clearly more immediate while cancer is more extended.
Both increases have continued and it can be surmised that once chlorination has been increased there is little effort to reduce it thereafter.
Both increases have continued and it can be surmised that once chlorination has been increased there is little effort to reduce it thereafter.
One way of looking at the effect of chlorine is to say that heart problems precede cancer as the body tries to protect itself, by using cholesterol as a defence against damaging ions produced by chlorination, but ultimately cannot adequately protect itself when those ions are changed to radicals by ioniation of metal water pipes.
The parallel incidence of heart disease and cancer can be further illustrated by the following graph which shows the rates of cancer and heart failure for District Health Boards (DHBs) in the North Island of New Zealand:
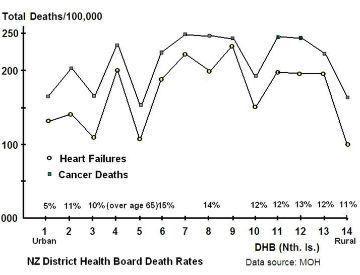
Again the parallel incidence of heart failure and cancer continues to be very clear.
The % of people over the age of 65 (where known) has been added to demonstrate that the parallel incidence of heart and cancer is much stronger than any relationship to age. I think we all know that cancer, at least, doesn't seem to be too picky when it comes to the age of its victims.
The % of people over the age of 65 (where known) has been added to demonstrate that the parallel incidence of heart and cancer is much stronger than any relationship to age. I think we all know that cancer, at least, doesn't seem to be too picky when it comes to the age of its victims.
Reducing heart failure and cancer within urban areas.
Publications.
The following list contains some of the theory, and some self help links:
Self help:
Alternatives to tap water
Build your own tank stand
Electrically isolated water distiller
Cancer patients and caregivers
Technical and other:
Acid buffer cancer hypothesis
Conductive water pipe case study Auckland
Asbestos cement water pipe hypocrisy
Ionisation of water pipes demonstrated
Tap water pH adjustment and heart disease
Water pipe deposits
Anti-cancer vaccine
Water pipe ionisation voltages
Research paper 2009
Related links:
Asbestos compensation
Website of Deidre van Gerven: fibreaware.org.nz
Latest material:
Masterton water which further links to the following (as well as related literature):
Submission to Masterton District Council
Submission addenda
Water Treatment update
Literature (also refer to Masterton water above):
Revis et al (Chlorine and cholesterol connection).
Rubenowitz et al (Magnesium).
Chambers (blood pH).
Yang et al (Chlorine and cancer connection).
Cancer Reports in pdf format: (these are in the National Library as hard copy)
Cancer Report 2007
Cancer Report 2008
Cancer Report 2009
Cancer Report 2010
Cancer Report 2011
Cancer Report 2012
(with a proposal for the attachment of water to guanine at C8).
Alternatives to tap water
Build your own tank stand
Electrically isolated water distiller
Cancer patients and caregivers
Technical and other:
Acid buffer cancer hypothesis
Conductive water pipe case study Auckland
Asbestos cement water pipe hypocrisy
Ionisation of water pipes demonstrated
Tap water pH adjustment and heart disease
Water pipe deposits
Anti-cancer vaccine
Water pipe ionisation voltages
Research paper 2009
Related links:
Asbestos compensation
Website of Deidre van Gerven: fibreaware.org.nz
Latest material:
Masterton water which further links to the following (as well as related literature):
Submission to Masterton District Council
Submission addenda
Water Treatment update
Literature (also refer to Masterton water above):
Revis et al (Chlorine and cholesterol connection).
Rubenowitz et al (Magnesium).
Chambers (blood pH).
Yang et al (Chlorine and cancer connection).
Cancer Reports in pdf format: (these are in the National Library as hard copy)
Cancer Report 2007
Cancer Report 2008
Cancer Report 2009
Cancer Report 2010
Cancer Report 2011
Cancer Report 2012
(with a proposal for the attachment of water to guanine at C8).
Research independence.
My research is not funded by any business or research organisation. Donations are welcome to defray costs (more information).
If you have a website of your own, you can help by adding a link to this site using the address http://www.cancer.net.nz/index.html Please pass the word around!
If you have a website of your own, you can help by adding a link to this site using the address http://www.cancer.net.nz/index.html Please pass the word around!
Summary.
We are led to believe that cancer and heart failure are completely different "diseases." I hope that this web site has demonstrated that the two are related conditions.
We are also led to believe that cancer is getting worse, that it's related to age, or diet, or exercise, or your grandmother's genes. These misconceptions miss the point that the cancer epidemic is quite specific to two environmental changes, both enshrined in legislation unique to post-war industrialised countries and both can be reversed or avoided.
The status of ions and radicals as causing disease needs to be on a par with bacteria and viruses. They are a normal part of the environment but in some circumstances are associated with illness because of an environmental change, a man-made change, which creates an effect which would not otherwise occur. In the case of cancer it is two environmental changes which conspire together to create the cancer epidemic and it is this interaction which has made the "cause" of the epidemic difficult to isolate.
The cancer epidemic has a clear starting point, as has the heart failure epidemic, and the simplest way to reverse both is by maintaining a buffer in water by improving filtration and by concurrently shutting off chemical dosing. The simplest way to avoid the epidemic personally is to use alternative clean water.
We are also led to believe that cancer is getting worse, that it's related to age, or diet, or exercise, or your grandmother's genes. These misconceptions miss the point that the cancer epidemic is quite specific to two environmental changes, both enshrined in legislation unique to post-war industrialised countries and both can be reversed or avoided.
The status of ions and radicals as causing disease needs to be on a par with bacteria and viruses. They are a normal part of the environment but in some circumstances are associated with illness because of an environmental change, a man-made change, which creates an effect which would not otherwise occur. In the case of cancer it is two environmental changes which conspire together to create the cancer epidemic and it is this interaction which has made the "cause" of the epidemic difficult to isolate.
The cancer epidemic has a clear starting point, as has the heart failure epidemic, and the simplest way to reverse both is by maintaining a buffer in water by improving filtration and by concurrently shutting off chemical dosing. The simplest way to avoid the epidemic personally is to use alternative clean water.
Stephen G. Butcher
cancer.debunk@yahoo.com
cancer.debunk@yahoo.com
My thanks to the developers of the following software:
Easy Graphic Converter 1.2
JPEGCompress 2.7
Jpegcrop 2004.06
Atlantis Nova 1.0.0.68
JPEGCompress 2.7
Jpegcrop 2004.06
Atlantis Nova 1.0.0.68

In some countries cancer and heart death rates have levelled off or have even reduced slightly. Two reasons for these reductions are:
(i) better control of residual chlorine and therefore less pH adjustment, and
(ii) replacement of older metal water pipes with plastic.
(i) better control of residual chlorine and therefore less pH adjustment, and
(ii) replacement of older metal water pipes with plastic.
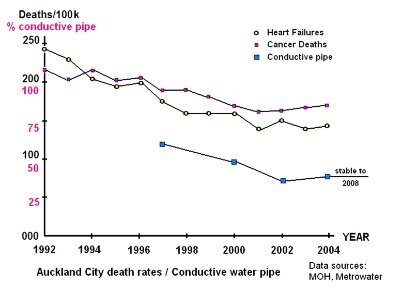
Here in New Zealand, the city of Auckland is one example of an urban area with reductions in heart failure and cancer rates which parallel reductions in conductive water pipes.
In the period 1992 - 2004 heart failures reduced around 40% and cancer deaths reduced around 20% and, as can be seen in the adjacent graph, the heart failure graph line crosses over cancer.
In the period 1992 - 2004 heart failures reduced around 40% and cancer deaths reduced around 20% and, as can be seen in the adjacent graph, the heart failure graph line crosses over cancer.
So, what's going on?
These hydronium exist as large structures rather than simply as water molecules with an extra hydrogen attached. The H3O+ cores form bonds with water molecules around them to create structures with strong bonds at the core and much weaker bonds to the water matrix. These weaker bonds to the matrix give the hydronium structures independence of movement. This means they can pass through cell walls much easier than water molecules, and also means that cholesterol is less effective as a defence against them.
Where to from here?
The causes of both epidemics relate to systems which are largely regulated by statute, and to change those statutes requires an admission that the laws controlling the adjustment of pH and the grounding of powerlines to water pipes are both faulty.
The major obstacle to this happening is caused by the way a water supply is deemed to be safe. That is, if it complies with the drinking water standards then it is "deemed" to be safe whether or not it is actually safe. There is no real time monitoring of the effects that water treatment changes have on public health and so no one is immediately aware of the adverse effects.
Moving from deeming water supplies to be legally safe, because they are compliant, to monitoring public health data to see if there are adverse effects is a major change that has to occur in civil service thinking.
I suppose it is convenient to think that "good" and "legally correct" are the same things, but it is so superficial as to be wrong!
So remedial work is likely to be incremental and slow unless there are sufficient water suppliers bold enough to make the necessary changes and create precedents which are seen to be unquestionably reproducible.
The major obstacle to this happening is caused by the way a water supply is deemed to be safe. That is, if it complies with the drinking water standards then it is "deemed" to be safe whether or not it is actually safe. There is no real time monitoring of the effects that water treatment changes have on public health and so no one is immediately aware of the adverse effects.
Moving from deeming water supplies to be legally safe, because they are compliant, to monitoring public health data to see if there are adverse effects is a major change that has to occur in civil service thinking.
I suppose it is convenient to think that "good" and "legally correct" are the same things, but it is so superficial as to be wrong!
So remedial work is likely to be incremental and slow unless there are sufficient water suppliers bold enough to make the necessary changes and create precedents which are seen to be unquestionably reproducible.
There is no reason why we cannot take responsibility for looking after ourselves by finding our own alternative safe water supplies.
I hope that in viewing this website you are sufficiently concerned and motivated to change your own circumstances and help others to do likewise.
In simple terms, a glass of treated water contains all it takes to trigger the cancer epidemic...
Stephen G. Butcher (B.Arch. Dip.BS)
email: cancer.debunk@yahoo.com
"Harwood," RD4 Masterton 5884, New Zealand
'phone: New Zealand 64 06 3727778
When hydronium ions pass through water pipes connected to electric power lines they, as positive ions, are subjected to negative ionisation because alternating current power lines will always negatively ionise.
Water absorbs carbon dioxide. This partially goes to carbonic acid in equilibrium, which is why water in it's natural state has an acid pH of around 6.5 to 6.8, i.e. slightly acid, rather than the theoretical 7.0 or neutral. When water has it's pH adjusted with lime, some of the calcium carbonate partially goes to carbonate and hydronium ions, increasingly so as the pH is forced further alkaline.
It seems probable, therefore, that hydronium ions would receive a single electron each as a result of this ionisation process and become hydronium radicals. They would then have a neutral charge, behave as if negatively charged, would be highly mobile within the bloodstream and across cell walls and would be highly damaging in relation to DNA replication leading to cancer.
Reversing the epidemics
Changes need to be made to water treatment and the electrical grounding of water pipes.
Reticulated water needs to be filtered down to around three microns for pathogen control, and chlorination must be stopped.
Water also needs to be buffered rather than pH adjusted. Buffering substitutes a strong acid with a weak one, keeps the pH within a range which is not harmful to life and avoids the production of hydronium. This occurs quite naturally if water is exposed to the air.
Water also needs to be buffered rather than pH adjusted. Buffering substitutes a strong acid with a weak one, keeps the pH within a range which is not harmful to life and avoids the production of hydronium. This occurs quite naturally if water is exposed to the air.
While the discontinuation of chlorination will stop both epidemincs, it would also be wise to isolate consumers' power supplies from ground and especially from metal water pipes. This process is presently underway here in New Zealand with circuits protected by RCDs not requiring bonding to earth. However, it must also be noted that while any power supply transformer is grounded rather than isolated then there will still be a capacitive connection to metal water pipes. If water pipes were equipotentially bonded to supply transformer earthing cables and to consumers' earths then ionisation might be prevented but it is not an ideal solution as it would also create earth loops which can play havoc with electrical equipment.
Cancer workbook for secondary schools
In 2010 I published a manual for senior secondary school pupils which covers the chemical and electrical processes of ionisation and includes an exercise in predicting heart failure rates using only pH and conductive pipe lengths as the variables. I may even get time to update it! The title is "Cancer, Heart Failure and what you can teach your teacher." ISBN 978-0-473-15543-8. Please email me for further information.
2011 and 2012 updates
My research was aided in 2011 by access to archived cancer registration data, and this has helped clarify the role of chlorination in the cancer epidemic.
The previous link to the submission to Masterton District Council incorporates much of my latest work and which more clearly identifies causal and interactive factors. It also provides an opportunity for Masterton residents to support the submission.
I've taken the plunge and in good faith have put forward a proposal on the joining of a water molecule to a guanine at C8. I have based that proposal on the epidemiology of the cancer epidemic. The proposal is deposited with the National Library of New Zealand, reference ISSN 1178-2994. An online version is posted above in the Cancer Report downloads section, or just click here.
The previous link to the submission to Masterton District Council incorporates much of my latest work and which more clearly identifies causal and interactive factors. It also provides an opportunity for Masterton residents to support the submission.
I've taken the plunge and in good faith have put forward a proposal on the joining of a water molecule to a guanine at C8. I have based that proposal on the epidemiology of the cancer epidemic. The proposal is deposited with the National Library of New Zealand, reference ISSN 1178-2994. An online version is posted above in the Cancer Report downloads section, or just click here.
( Links updated 13/07/12, revised 22/09/12, new hit counter 13/12/12.)
(Revised 16/03/13)
(Revised 16/03/13)
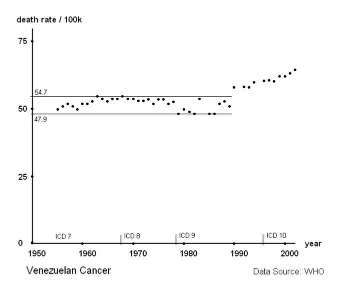
Venezuela illustrates the way in which the heart failure and cancer epidemics are related, that is, they are the result of common environmental factors and are not separate diseases.
This is an important concept to grasp: that the cancer epidemic shares a common causal factor with the heart failure epidemic. Therefore both epidemics can be stopped in one go by discontinuing chlorination.
This is an important concept to grasp: that the cancer epidemic shares a common causal factor with the heart failure epidemic. Therefore both epidemics can be stopped in one go by discontinuing chlorination.
So, adjusting water pH with lime has a similar effect as adding chlorine: both processes create hydronium ions.
Rainwater would be the first choice for a safe drinking water supply because it is buffered (although rainwater is becoming increasingly polluted by the burning of plastic waste with increased risk of leukaemia...). Extracting water from bores and taking care not to reticulate the water in metal pipes, and allowing the water time to absorb or release carbon dioxide in a storage or header tank, is another viable option.
If there is doubt about bugs in the water, filtration down to 3 microns would suffice.
It may be that the most practical option is to move to a rural location.
If there is doubt about bugs in the water, filtration down to 3 microns would suffice.
It may be that the most practical option is to move to a rural location.
So we can see that cancer risk is directly related to the town or city of domicile. In New Zealand, people who live in Wanganui (291/100k) have twice the risk of dying from cancer as people who live in Wellington (148/100k), and people who live and work in the country have minimal risk. Now, that is worth knowing!
Logically, one way to reduce heart failure and cancer risk is to move from high risk areas, that is, live and work in the country. On the other side of the coin, one way for TLAs to retain or grow populations is to face up to the epidemiology and upgrade their water supplies.
Logically, one way to reduce heart failure and cancer risk is to move from high risk areas, that is, live and work in the country. On the other side of the coin, one way for TLAs to retain or grow populations is to face up to the epidemiology and upgrade their water supplies.
| TLA, North Island, NZ | Death Rate (per 100k) |
| Control (no epidemic) | 56 |
| Wellington | 148 |
| Hamilton | 169 |
| Palmerston North | 180 |
| Auckland | 181 |
| Hutt City | 192 |
| Hastings | 208 |
| Taupo | 212 |
| Rotorua | 214 |
| Whangarei | 215 |
| Tauranga | 228 |
| Masterton (see next) | 232 |
| New Plymouth | 236 |
| Napier | 242 |
| Gisborne | 245 |
| Wanganui | 291 |
Changes to piping infrastructure and electrical codes take time and expense. Auckland is an example where some of this remedial work has been done, albeit for reasons other than cancer control, and the work has been spread over a number of years and undoubtedly would have been at some expense.
An infinitely faster and less expensive approach is as I have suggested, that is, to improve the filtration in the water treatment process so that the chemical processes of chlorination and pH adjustment can be turned off without adverse effect on public health.
An infinitely faster and less expensive approach is as I have suggested, that is, to improve the filtration in the water treatment process so that the chemical processes of chlorination and pH adjustment can be turned off without adverse effect on public health.
The cancer epidemic began after 1950 and only affects some countries. It is switched on by the chlorination of drinking water, is man-made and is totally preventable.
Water treatment philosophies date back to the cholera epidemics of the mid 1800s. These were caused by bacteria from sewage getting into water supplies. Rather than maintaining clean water supplies it was found expedient, and cheap, to kill faecal and other bacteria by dosing with chlorine. However chlorine dosing, being strongly acid, corroded metal water pipes and copper fittings. Lime was added, and still is, to make the water alkaline and reduce corrosion. However, adjusting the pH of water outside its normal range creates unpaired ions in the water which forces an increase in cholesterol production in people as a defence. This, in turn, leads to ischaemic heart failure through oxygen starvation.
The heart failure epidemic preceded the cancer epidemic, historically, by about 50 years, the heart failure epidemic beginning around the early 1900s, and continuing today. Around 1950 it became mandatory in industrialised countries to connect water pipes to power lines. This connection is made by linking the neutral conductor to water pipes in consumers' homes. However, there is no link where the water pipes pass electricity supply transformers. This has the effect of ionising metal water pipes and altering the unpaired ions formed by pH adjustment, giving them a negative charge and creating radicals leading to cancer.
The heart failure epidemic preceded the cancer epidemic, historically, by about 50 years, the heart failure epidemic beginning around the early 1900s, and continuing today. Around 1950 it became mandatory in industrialised countries to connect water pipes to power lines. This connection is made by linking the neutral conductor to water pipes in consumers' homes. However, there is no link where the water pipes pass electricity supply transformers. This has the effect of ionising metal water pipes and altering the unpaired ions formed by pH adjustment, giving them a negative charge and creating radicals leading to cancer.
I've added in the control or baseline "no epidemic" rate and, as you can see, New Zealand is definitely in the grips of a "grand mal" epidemic.
We can see that in Whanganui the risk of cancer is twice as high as it is in Wellington. That sort of difference simply cannot be explained away in terms of ethicity, aging population or other long shot excuse.
There is a Cancer Atlas for New Zealand which shows the distribution of cancers throughout the country but it avoids the data you see here. It limits itself to cancer type, gender and ethnicity rather than relating cancer incidence in any way to where a person might live, i.e. it deals in averages rather than specifics.
We can see that in Whanganui the risk of cancer is twice as high as it is in Wellington. That sort of difference simply cannot be explained away in terms of ethicity, aging population or other long shot excuse.
There is a Cancer Atlas for New Zealand which shows the distribution of cancers throughout the country but it avoids the data you see here. It limits itself to cancer type, gender and ethnicity rather than relating cancer incidence in any way to where a person might live, i.e. it deals in averages rather than specifics.
The simplest and quickest way to end the epidemic is by discontinuing the chlorination of drinking water and replacing chlorination with filtration.
Not all countries have a cancer epidemic! Rather than cancer being a global problem, the epidemic is localised to most industrialised countries. When people move between countries their risk of getting cancer changes according to the country in which they live.
And again, within territorial areas there is a clear difference between urban and rural cancer rates. Looking at the Masterton District (TLA) from the chart above we can see that cancer registration rates vary considerably:
| Domicile Area (1998 - 2008) |
Registrations (per 100k) |
| Control (no epidemic) | 112 |
| Masterton urban | 783 |
| Kopuaranga | 94 |
| Opaki | 566 |
| Homebush/Te Ore Ore | 332 |
| Whareama (see next) | 193 |
So, why the big difference between urban and rural? Very simply it depends on the water supply. In the case of Masterton, the rural area of Kopuaranga has no water supply and the lowest cancer registration rate. Opaki and Homebush have unchlorinated water supplies but many residents work in the Masterton urban area.
If we take an even closer look, this time at Whareama, we can see the effect of stopping chlorination:
| Whareama Registration Date |
Registrations (actual) |
| 1983-1986 | 25 |
| 1987-1990 | 27 |
| 1991-1994 | 26 |
| 1995-1998 | 22 |
| 1999-2002 | 26 |
| Chlorinator disconnected | variable |
| 2005-2008 | 13 |
This illustrates the result of removing chlorination, that is, cancer registrations halve when chlorination is discontinued. This is the opposite of adding chlorine, which doubles cancer registration rates. I have excluded a 2 year window, 2003 and 2004, from the table and it is within this window, really the first 12 months, that registration rates halve.
There is another effect which chlorination has prior to the presentation of cancer, and that is the effect it has on the incidence of ischaemic heart failure. Chlorination began in the early 1900s and is causal to the heart failure epidemic. The cancer epidemic didn't start at the same time because chlorination alone cannot cause cancer.
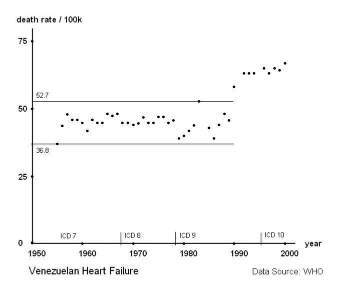
Chlorination, as a causal factor, requires a second interactive factor in order to cause cancer. That interactive factor is the connection of electric power lines to metal water pipes. Where the interactive factor already exists, heart failure and cancer registrations increase at the same time. For example, Venezuala follows the US Electric Wiring Rules and already had the interactive factor, so both cancer and heart failure rates increased together:
Chlorination, as a causal factor, requires a second interactive factor in order to cause cancer. That interactive factor is the connection of electric power lines to metal water pipes. Where the interactive factor already exists, heart failure and cancer registrations increase at the same time. For example, Venezuala follows the US Electric Wiring Rules and already had the interactive factor, so both cancer and heart failure rates increased together:
Heart failure is a precursor to cancer
Masterton residents can click on this link, Masterton_water, for a layman's summary.
New cancer treatments are not the only answer. While having more tools in the toolbox is great, it is foolish to think that this path can turn back the cancer epidemic. Invariably a vast resource of funding is available for this purpose but it ignores the fundamental question, how can you find a cure without first finding the cause, except you find the cure by accident?
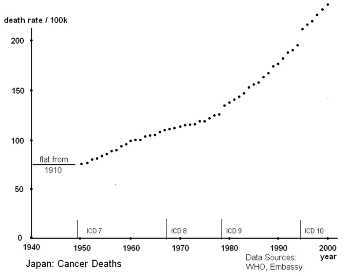
As a confounder, that is another factor which appears to muddy the waters, lowering cholesterol through diet increases cancer incidence. Cultures which have less "bad cholesterol" or which include largish amounts of catechins, e.g. green tea and red wine acting in such a way as to inhibit platelet function, display a much higher increase in cancer incidence increases than do other cultures.
Japan is one example. Singapore is not dissimilar. France is another, with the so-called French Paradox related to red wine consumption which reduces ischaemic heart failure.
The graph for cancer deaths in Japan shows just how dramatic the increase has been since reconstruction after WW2. The prewar incidence of cancer was exemplary but is now looking to outstrip the rest of the industrial world.
The graph for cancer deaths in Japan shows just how dramatic the increase has been since reconstruction after WW2. The prewar incidence of cancer was exemplary but is now looking to outstrip the rest of the industrial world.
History leading up to the epidemic
Age groups affected by cancer
As must be apparent, cancer is shifting forward and is no longer the reserve of the elderly. Studies have shown that the biggest increases in cancer are in those people in their fifties, so it is families who are now being greatly affected.
The link to Masterton_water for Masterton residents or the direct link to Water_treatment_update contains some useful data on this most devastating effect.
The link to Masterton_water for Masterton residents or the direct link to Water_treatment_update contains some useful data on this most devastating effect.